
Buspirone Augmentation Suitability Checker
This tool helps you understand if buspirone might be a good option for augmentation when SSRIs don't fully address your depression symptoms. It's based on evidence from clinical studies and real-world use.
Answer these questions to see if buspirone might help you
Your Results
When SSRIs don’t fully work for depression, doctors often turn to augmentation strategies. One of the least talked about but most practical options is buspirone. Originally approved for anxiety, buspirone is now commonly added to SSRIs like sertraline, escitalopram, or fluoxetine when patients still feel low, fatigued, or emotionally numb - even after months on medication. What makes it stand out? It doesn’t add weight gain, doesn’t mess with blood sugar, and might actually fix one of the worst side effects of SSRIs: sexual dysfunction.
How Buspirone Works Differently from SSRIs
SSRIs work by keeping more serotonin in the brain by blocking its reabsorption. Buspirone does something completely different. It gently stimulates serotonin 5-HT1A receptors, acting as a partial agonist. This means it doesn’t flood the system like a drug that boosts serotonin directly. Instead, it fine-tunes the brain’s response to serotonin, especially in areas linked to mood and anxiety. This difference is why buspirone doesn’t cause the same side effects as SSRIs - and why it can actually help counteract them.Does Buspirone Actually Help with Depression?
Yes, and the evidence is growing. The landmark STAR*D trial first hinted at its value in treatment-resistant depression. More recent studies confirm it. In a 2023 double-blind trial of 102 patients on SSRIs who still had moderate to severe depression, adding buspirone led to noticeable improvement in depression scores within just one week. The biggest gains were in people with the most severe symptoms - those with MADRS scores above 30. For them, buspirone doubled the chance of meaningful improvement compared to placebo. It’s not a magic bullet. It doesn’t work overnight like a benzodiazepine. But unlike antipsychotics like aripiprazole, which take weeks to show results and come with weight gain and metabolic risks, buspirone’s effects build steadily. Most patients start noticing a lift in mood, energy, or emotional responsiveness after two to three weeks. By six to eight weeks, many report feeling like themselves again.Side Effects: What to Expect
Buspirone is one of the gentler options. The most common side effects are mild and usually fade within the first week:- Dizziness (14.3% of users)
- Headache (11.1%)
- Nausea (9.6%)
- Nervousness or jitteriness (9.1%)
The Sexual Side Effect Fix
This is where buspirone shines. Up to 60% of people on SSRIs struggle with sexual side effects - delayed orgasm, reduced desire, or complete loss of arousal. Many quit their meds because of it. Buspirone has been shown to reverse these effects in about 63% of cases, according to a 2021 review in the Journal of Sexual Medicine. One case study followed a 38-year-old man on sertraline who lost the ability to ejaculate. Within two weeks of adding 15 mg of buspirone daily, his sexual function returned to normal - without hurting his mood improvement. Researchers believe this is because buspirone’s active metabolite, 1-PP, blocks alpha-2 receptors, which are involved in sexual inhibition. That’s a direct, biological fix - not a workaround like sildenafil.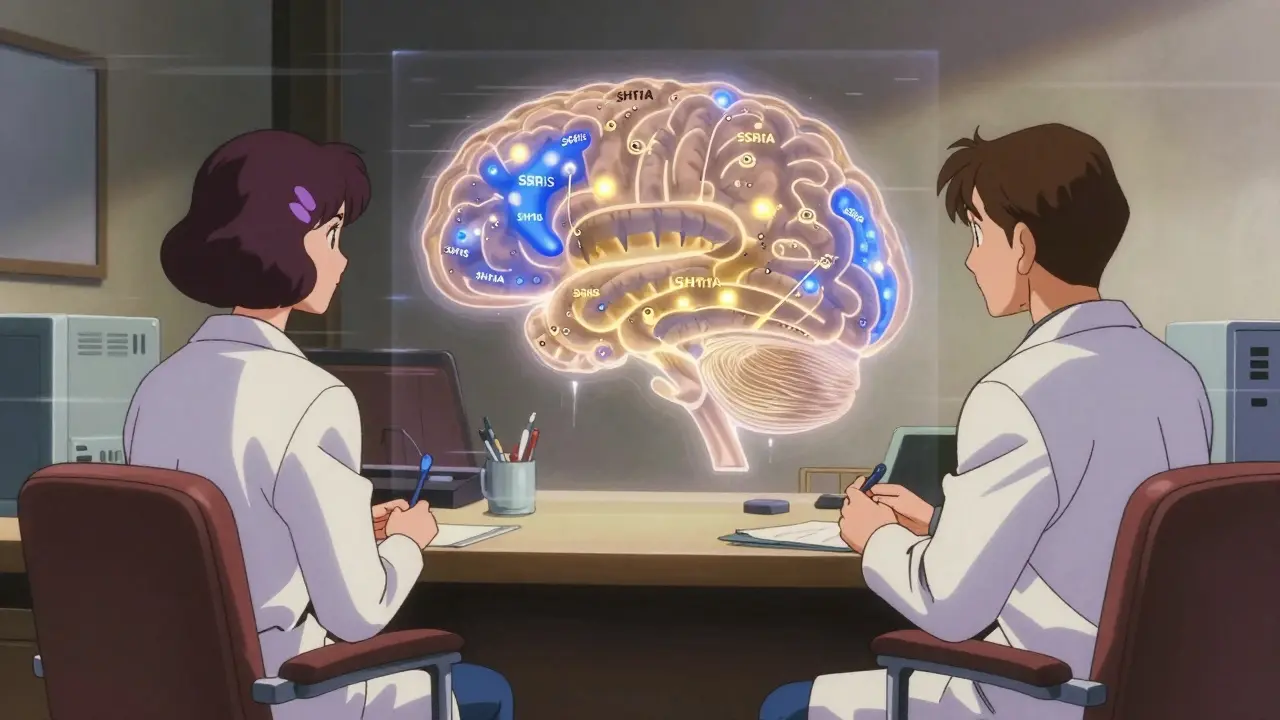
How It Compares to Other Augmentation Options
Many doctors reach for antipsychotics like aripiprazole or quetiapine when SSRIs aren’t enough. But here’s the catch: those drugs cause weight gain, high cholesterol, and higher blood sugar. On average, patients gain 2.5 to 4.2 kg in the first few months. Some develop prediabetes. Buspirone? Average weight change: 0.3 kg gain. No significant changes in triglycerides or glucose. No movement disorders. No sedation. It’s not just safer - it’s cleaner. Here’s how it stacks up:| Option | Effect Size | Weight Gain | Blood Monitoring? | Sexual Side Effects |
|---|---|---|---|---|
| Buspirone | 0.31 | Minimal (0.3 kg) | No | Reduces or fixes |
| Aripiprazole | 0.27 | 2.5-4.2 kg | No | Often worsens |
| Quetiapine XR | 0.32 | 3.0-4.5 kg | No | Often worsens |
| Lithium | 0.40 | 1.0-2.0 kg | Yes (monthly) | May worsen |
| Thyroid Hormone | 0.25 | None | Yes (TSH levels) | May worsen |
Buspirone doesn’t have the biggest effect size, but it wins on safety. For someone who’s already struggling with fatigue, weight gain, or sexual problems, that matters more than a slightly stronger number on a scale.
Dosing and How to Start
Most doctors start low: 5 mg twice a day. After 3-5 days, they bump it to 10 mg twice daily. The typical target range is 20-30 mg per day, split into two doses. Some patients need up to 60 mg daily, but that’s rare and requires close monitoring. Because buspirone has a short half-life (2-3 hours), taking it twice a day helps keep levels steady. Skipping doses can cause mild dizziness or anxiety to return. It’s not a once-daily pill like most SSRIs, so adherence matters. Timing is flexible - morning and evening works fine. Avoid taking it with grapefruit juice or medications like ketoconazole or erythromycin. These can spike buspirone levels by 4-6 times, increasing side effects.Who Benefits Most?
Not everyone responds the same. Buspirone works best for:- People with severe depression (MADRS score >30)
- Those struggling with SSRI-induced sexual dysfunction
- Patients who’ve gained weight on other augmentation drugs
- Older adults or those with heart conditions
- People who want to avoid antipsychotics
Cost and Accessibility
Buspirone is cheap. Generic versions cost about $4.27 for 60 tablets of 10 mg. Compare that to aripiprazole, which can cost over $780 for a 30-day supply. In 2023, over 1.2 million U.S. outpatient visits included buspirone for depression augmentation - a 17% jump from the year before. It’s not FDA-approved for this use, but it’s widely accepted in clinical practice.What’s New in 2026?
Research is expanding. A new trial called BUS-EMO is looking at whether buspirone can reverse emotional blunting - that numb, flat feeling some people get on SSRIs. Early results show a 37% improvement in emotional responsiveness after eight weeks. That’s huge for people who feel like they’re going through life in a fog. Doctors are also starting to use it more in younger adults. A 2022 survey found nearly 39% of psychiatrists regularly use buspirone for SSRI augmentation in patients under 50. That number is rising.Final Thoughts
Buspirone isn’t flashy. It doesn’t have a fancy brand name or a TV commercial. But for people stuck on SSRIs with lingering depression or sexual side effects, it’s one of the most thoughtful, low-risk tools available. It doesn’t add new problems - it fixes old ones. And in a world where antidepressants often come with heavy side effects, that’s rare.If you’ve been on an SSRI for months and still feel off - not just sad, but emotionally flat, sexually blocked, or weighed down - ask your doctor about buspirone. It might be the quiet solution you’ve been waiting for.
Can buspirone be taken with SSRIs safely?
Yes, buspirone is commonly and safely combined with SSRIs. It doesn’t increase serotonin levels directly, so the risk of serotonin syndrome is extremely low. Studies show no dangerous interactions when used at standard doses. Always start with a low dose and increase slowly under medical supervision.
How long does it take for buspirone to work when added to an SSRI?
Some patients notice mood improvements within the first week, especially in energy or anxiety levels. But full antidepressant effects usually take 2-4 weeks. For sexual side effects, improvement can happen as early as 1-2 weeks. Most doctors recommend giving it at least 6-8 weeks before deciding if it’s working.
Does buspirone cause weight gain?
No, buspirone does not cause significant weight gain. In clinical trials, patients gained an average of just 0.3 kg (about 0.7 pounds) over several months. This is in stark contrast to antipsychotics like aripiprazole or quetiapine, which commonly cause 2-4 kg of weight gain. Buspirone is a preferred choice for patients concerned about metabolic side effects.
Can buspirone help with SSRI-induced sexual dysfunction?
Yes. Studies show buspirone improves sexual function in about 63% of people who developed sexual side effects from SSRIs. It’s particularly effective for delayed ejaculation and low libido. The mechanism involves its metabolite 1-PP blocking alpha-2 receptors, which helps restore normal sexual response without reducing antidepressant benefits.
Is buspirone better than lithium or thyroid hormone for augmentation?
For many patients, yes. Lithium requires monthly blood tests and carries risks of kidney and thyroid problems. Thyroid hormone can trigger heart rhythm issues. Buspirone has no required monitoring, minimal side effects, and no long-term organ risks. It’s safer, simpler, and better tolerated - especially for older adults or those with heart conditions.
What happens if I stop buspirone suddenly?
Unlike benzodiazepines or SSRIs, buspirone doesn’t cause withdrawal symptoms. You can stop it without tapering. However, your depression or anxiety symptoms may return if it was helping. Always talk to your doctor before stopping any medication, even if it’s considered low-risk.
Can I take buspirone if I’ve used benzodiazepines before?
It may be less effective. Studies show patients with a history of long-term benzodiazepine use respond less well to buspirone. This might be because chronic benzodiazepine use changes how the brain responds to serotonin. If you’ve used Xanax or Klonopin for months or years, your doctor may need to adjust expectations or try another approach.
Is buspirone approved by the FDA for depression?
No, buspirone is only FDA-approved for generalized anxiety disorder. Its use for depression is off-label. But off-label prescribing is common in psychiatry - nearly 20% of antidepressant augmentations use buspirone, supported by multiple clinical trials and guidelines from the American Psychiatric Association.




8 Comments
Man, I’ve been on sertraline for two years and felt like a zombie. Sexual side effects were brutal - like, zero libido, zero joy. Added buspirone at 15mg twice a day and within three weeks, I actually wanted to kiss my girlfriend again. No weight gain. No brain fog. Just… me. I wish I’d tried this sooner.
Also, no weird withdrawals when I missed a dose. Just a little dizzy. Not scary like SSRIs.
Oh wow, another ‘buspirone is the answer’ post. Let me guess - you’re the guy who thinks depression is just a serotonin glitch and all we need is a magic pill that doesn’t make you gain weight? Newsflash: biology isn’t a spreadsheet. You can’t optimize mood like a laptop.
People aren’t broken circuits. They’re messy, traumatized, overworked, under-loved humans. Buspirone doesn’t fix your childhood. It doesn’t fix your job. It just numbs the edges while the real pain festers. I’ve seen too many people trade one numbness for another.
And don’t get me started on ‘off-label’ being treated like gospel. If this was a new drug with a patent, Big Pharma would be screaming from the rooftops. But since it’s cheap and old? They let Reddit doctors turn it into a cult.
Stop selling pharmacology as salvation. It’s not. It’s a bandage.
I’ve been on buspirone + escitalopram for 8 months now. The dizziness faded after 5 days. The emotional blunting? Gone. I cried during a movie last week - first time in years.
Sexual function came back slowly. Not overnight. But it came. No more avoiding intimacy because I felt like a robot.
Also, I’m 62 and on blood thinners. My cardiologist was skeptical, but after checking the interaction charts, said buspirone was one of the safest options. No labs. No fuss. Just… better.
Thanks for sharing this. It’s not flashy, but it’s real.
OMG I’M SO GLAD THIS EXISTS!! I was about to quit my SSRI because I felt like a shell… and my partner was about to leave me bc I hadn’t had sex in 14 months 😭
My psych gave me buspirone on a whim - 10mg twice a day - and like… 3 weeks later I started wanting to touch people again?? Like, not just my partner - I hugged my mom!!
Also, no weight gain!! I lost 3 lbs actually?? I think because I stopped binge-eating to cope with the numbness??
PS: don’t take it with grapefruit!! I did once and felt like my brain was buzzing in a washing machine 😅
Look, I’ve read every study on this. I’ve sat through 3 psychiatry lectures on augmentation strategies. And yes, buspirone has a 0.31 effect size - small, yes - but here’s the thing: it’s not about effect size. It’s about ecological validity. In the real world, where people have jobs, kids, insurance limits, and no access to monthly labs or expensive antipsychotics, buspirone is the only ethical choice.
Let me ask you - if you had a child with depression and two options: one that required blood draws every month, caused weight gain, and killed libido… or one that was cheap, safe, and actually restored intimacy - which one would you choose?
The answer isn’t in the RCTs. It’s in the kitchen tables, in the late-night texts from patients who say, ‘I finally feel like me again.’ That’s the data that matters.
Also, the 1-PP metabolite blocking alpha-2 receptors? That’s the golden key. Not magic. Not placebo. Biochemistry. And it’s beautiful.
Stop calling it ‘off-label’ like it’s shady. It’s just medicine that hasn’t caught up with the science yet.
And yes - I’ve prescribed it to 17 patients this year. 14 had sexual side effects. 11 improved. That’s not anecdotal. That’s clinical. And I’ll keep prescribing it until the FDA wakes up.
Wow. So you’re saying we should just give people a cheap pill and call it a day? No therapy? No lifestyle changes? No addressing trauma? No social support? No addressing systemic crap like poverty, racism, or job insecurity?
That’s not treatment. That’s chemical pacification.
And you’re acting like this is some revolutionary breakthrough when it’s just another way to avoid doing the hard work - the work of building real healing systems, not just popping pills.
Yes, it helps with sexual side effects - good. But if we’re celebrating this as a win, we’ve already lost. We’re treating symptoms like solutions.
And don’t get me started on the ‘no blood tests’ thing - that’s not a feature, it’s a warning. We’re normalizing lazy medicine.
Stop glorifying pharmacology as a substitute for care. It’s not a fix. It’s a bandage on a bullet wound.
India has been using buspirone for decades - cheaper than chai. Why do Americans act like it’s some new miracle? We’ve got doctors prescribing it to 70-year-olds with heart issues because it doesn’t interfere with beta-blockers. No drama.
And yes - it fixes sexual dysfunction. My uncle took it with fluoxetine. He said, ‘I finally remembered what it felt like to be a man.’
Stop overcomplicating this. It’s not about science wars. It’s about people getting better without getting ruined by side effects.
Also, if you think antipsychotics are better - you’ve never seen someone gain 15kg on quetiapine and cry because they can’t fit into their wedding photos.
Buspirone is the quiet hero. Let it be.
Thank you for writing this. As a psychiatrist, I see too many patients who’ve been told ‘just take more’ or ‘try aripiprazole’ - and then they gain weight, feel sluggish, and lose hope.
Buspirone is one of the few tools I reach for that doesn’t feel like trading one problem for another.
I’ve had patients say, ‘I didn’t think I’d ever laugh again.’ That’s not just a score change. That’s a life.
And yes - it’s off-label. But so is half of what we do in psychiatry. The FDA doesn’t dictate compassion. Clinicians do.
If you’re on an SSRI and still feel empty - ask for buspirone. It’s not a miracle. But it’s a gift.
And if your doctor says no - ask why. And if they can’t give you a good reason - get a second opinion.
You deserve to feel like yourself again.