That sharp catch in your hip when you stand up from a low chair? Or the deep ache that lingers after a long drive? If you’re dealing with this, you aren’t just imagining things. Hip pain is complex because it often involves two distinct but connected problems: labral tears areruptures in the fibrocartilage ring that seals the hip joint, acting as shock absorbers, while hip osteoarthritis isthe progressive wear-and-tear of the articular cartilage surface. For years, doctors treated these separately. Today, experts like Dr. Brian White at Western Orthopaedics recognize them as a bidirectional relationship-where one condition can accelerate the other. The good news? You don’t always need surgery to find relief. Strategic activity modification can change the trajectory of your pain.
Understanding the Mechanics: Why Your Hip Hurts
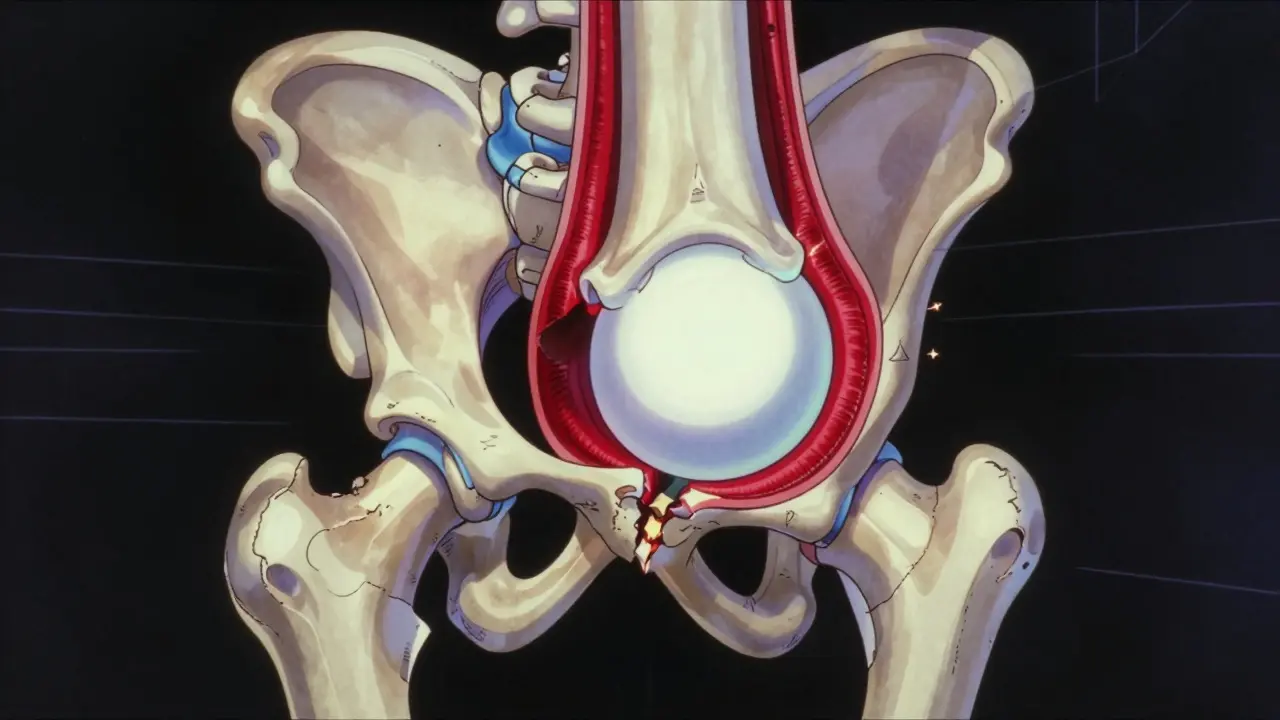
To fix the problem, we first need to understand what’s broken. Think of your hip socket (acetabulum) as a cup and your thigh bone head (femur) as a ball. The hip labrum isa 3-5mm thick fibrocartilaginous structure forming a complete ring around the acetabular rim. It isn’t just padding; it’s a suction seal. Biomechanical studies show it maintains negative intra-articular pressure, keeping the joint stable. When this seal tears, contact stress on the actual cartilage increases by 92%.
This instability often stems from Femoroacetabular Impingement (FAI) isa structural abnormality where excess bone causes friction in the hip joint. There are three types:
- Cam-type (64% of cases): Extra bone on the femoral head-neck junction. This acts like a wedge, grinding against the labrum during flexion.
- Pincer-type: Overcoverage of the acetabulum, crushing the labrum between the socket and ball.
- Mixed-type: A combination of both.
If left unchecked, this grinding leads to Hip Osteoarthritis (OA) isdegenerative joint disease characterized by cartilage loss and bony changes. Research shows 70-90% of patients with FAI have associated labral pathology. Meanwhile, 54% of those with established OA also have labral tears. They feed each other. A torn labrum reduces synovial fluid retention by 40-60%, accelerating cartilage wear in weight-bearing zones.
The Diagnostic Gap: Imaging vs. Reality
Here is where many patients get stuck. You might have an MRI showing a "torn labrum," but does that explain your pain? Not necessarily. Dr. David M. Walton’s team at Yale Medicine found that 38% of asymptomatic individuals over 50 have labral tears on MRI. Just because it’s there doesn’t mean it’s the primary pain generator.
Clinicians now use a more nuanced approach. They look for specific mechanical signs rather than relying solely on images. Key diagnostic indicators include:
- The FADIR Test: Flexion, Adduction, and Internal Rotation. If this reproduces your exact groin pain, it suggests impingement or labral irritation.
- Alpha Angle Measurement: On MRI, an alpha angle greater than 55 degrees indicates cam-type FAI.
- Kellgren-Lawrence Grading: Radiologists grade OA from 0 (no evidence) to 4 (severe joint space narrowing <2mm).
Dr. Thomas P. Vail from UCSF warns against overemphasizing labral pathology in older patients. If you are over 60 with global cartilage loss (Grade 3-4 OA), fixing the labrum alone rarely solves the problem because the underlying cushion is gone.

Activity Modification: The First Line of Defense
Surgery isn’t the only answer. In fact, for many, conservative management is superior initially. The goal isn’t to stop moving-it’s to move differently. The Cleveland Clinic’s 2023 protocol recommends a structured 4-6 week modification period. Here is how you apply it in real life:
| Activity | Risk Factor | Modification Strategy |
|---|---|---|
| Sitting at a Desk | Hip flexion >90 degrees for prolonged periods | Use a wedge cushion to tilt pelvis forward; stand every 30 minutes |
| Sleeping | Internal rotation and adduction | Place a pillow between knees to maintain neutral alignment |
| Driving | Deep hip flexion and internal rotation | Adjust seat further back; use a lumbar roll to reduce pelvic tilt |
| Squats/Lunges | Combined flexion and internal rotation | Switch to split squats with external rotation cue; limit depth to 45 degrees |
| Yoga/Pilates | Extreme end-range positions (e.g., Pigeon Pose) | Avoid poses requiring >90 degree flexion; focus on glute activation |
Data from the Arthritis Foundation supports this. Among 1,247 respondents, 92% reported significant improvement by eliminating deep squats and lunges. Another 87% found relief by avoiding sitting cross-legged. These aren’t minor tweaks; they remove the mechanical pinch causing the inflammation.
Treatment Options: From Injections to Surgery
If activity modification doesn’t cut it, what’s next? The path depends heavily on your age, activity level, and the severity of cartilage damage.
Conservative Care
Physical therapy is the cornerstone. Studies show success rates jump to 85% when patients learn to identify their specific "pain provocation positions." Therapists focus on strengthening hip abductors to control femoral motion. NSAIDs (like ibuprofen 400-800mg) help manage acute inflammation, but they don’t fix the mechanics.
Injections
Corticosteroid injections providetemporary anti-inflammatory relief lasting an average of 3.2 months. They work for 68% of patients, but caution is needed. Repeated use (more than three per year) carries a 12% risk of cartilage damage. Viscosupplementation (Hyaluronic Acid) offerslubrication for the joint, with modest 15-20% pain reduction in 55% of patients. However, effects diminish after six months. Newer options like Durolane (FDA approved 2023) may extend this duration to six months.
Surgical Intervention
When non-surgical methods fail, surgery becomes an option. But which type?
- Labral Repair: Suturing the torn tissue back to the bone. Satisfaction rates are 85-92% at five years. This preserves the seal.
- Labral Debridement: Trimming the torn tissue. Satisfaction drops to 65-75%. It removes pain generators but loses the suction effect.
- Total Hip Arthroplasty (THA): Replacing the entire joint. Reserved for advanced OA (Grade 4). About 450,000 Americans undergo this annually.
For younger patients with cam-type FAI (alpha angle >55 degrees), surgical correction plus repair yields 73% better outcomes than conservative care alone. However, for patients over 60 with established OA, progression to THA occurs in 45% of cases within five years regardless of initial intervention.

Real-World Implementation: Avoiding Movement Phobias
A major pitfall in managing hip pain is becoming afraid to move. Dr. Vail cautions that creating "movement phobias" leads to deconditioning, which worsens outcomes. The key is quality over quantity.
Consider the case of a 45-year-old yoga instructor documented by the Cleveland Clinic. She didn’t quit yoga. She modified it. By reducing hip flexion beyond 90 degrees and eliminating pigeon pose, she achieved 70% pain reduction in three months without surgery. This illustrates the power of targeted adaptation.
Workplace ergonomics play a huge role too. 78% of office workers struggle with prolonged sitting. Simple tools help:
- Raised Toilet Seat: Reduces hip flexion by 15-20 degrees during use.
- Wedge Cushion in Car: Decreases hip flexion by 10-15 degrees while driving.
- Standing Desks: Alternate sitting and standing to prevent static load accumulation.
Recent innovations offer hope. A 2023 pilot study at Stanford University used wearable sensor technology to provide real-time feedback on hip positioning. Participants reduced pain episodes by 52% over 12 weeks. While not yet standard care, it highlights the future of biofeedback-driven rehabilitation.
When to See a Specialist
You should consult an orthopedic specialist if:
- Pain persists despite 4-6 weeks of consistent activity modification and physical therapy.
- You experience locking, catching, or giving way sensations in the hip.
- Night pain disrupts sleep consistently.
- Walking distance decreases significantly (claudication-like symptoms).
Don’t wait until you’re limping. Early intervention with activity modification and targeted PT can delay progression to surgery by 3.5-5 years in 65% of patients with mild-to-moderate pathology. Time is cartilage.
Can a labral tear heal on its own?
The labrum has very poor blood supply, so true biological healing is rare. However, symptoms can resolve significantly through scar tissue formation and improved biomechanics via physical therapy. Many patients achieve functional recovery without the tear physically "healing" in the traditional sense.
Is hip arthroscopy safe for older adults?
Safety depends on the underlying cartilage status. For patients over 60 with significant osteoarthritis (Kellgren-Lawrence Grade 3-4), arthroscopy often fails to provide lasting relief and may accelerate the need for total hip replacement. It is generally reserved for younger patients or those with isolated labral tears and healthy cartilage.
What exercises should I avoid with a labral tear?
Avoid movements that combine deep hip flexion (>90 degrees) with internal rotation. This includes deep squats, lunges, kneeling, sitting cross-legged, and yoga poses like Pigeon or Butterfly. High-impact activities like running may also aggravate symptoms if gait mechanics are compromised.
How long does recovery take after labral repair surgery?
Recovery is gradual. Most patients use crutches for 4-6 weeks. Return to daily activities takes 3-4 months, while return to high-level sports or heavy labor can take 6-9 months. Adherence to post-operative restrictions is critical for graft healing.
Does weight loss help hip pain?
Yes. Every pound of body weight places approximately 3-4 pounds of additional force on the hip joint during walking. Weight loss reduces mechanical load and systemic inflammation, potentially slowing the progression of osteoarthritis and improving pain levels.

Write a comment