Your arm feels heavy. Reaching for a seatbelt or scratching your back becomes a painful chore. At night, the ache keeps you awake. If this sounds familiar, you might be dealing with frozen shoulder, medically known as adhesive capsulitis. It is not just "stiffness." It is a specific condition where the tissue capsule surrounding your shoulder joint thickens and tightens, trapping the joint in place.
The good news? Frozen shoulder is self-limiting. This means it will eventually resolve on its own. The bad news? That natural process can take anywhere from one to three years. However, targeted mobilization strategies can cut that recovery time significantly, often reducing it to six to twelve months. Knowing exactly how to move-and when to stop-is the difference between speeding up healing and making inflammation worse.
Understanding Adhesive Capsulitis: What Is Actually Happening?
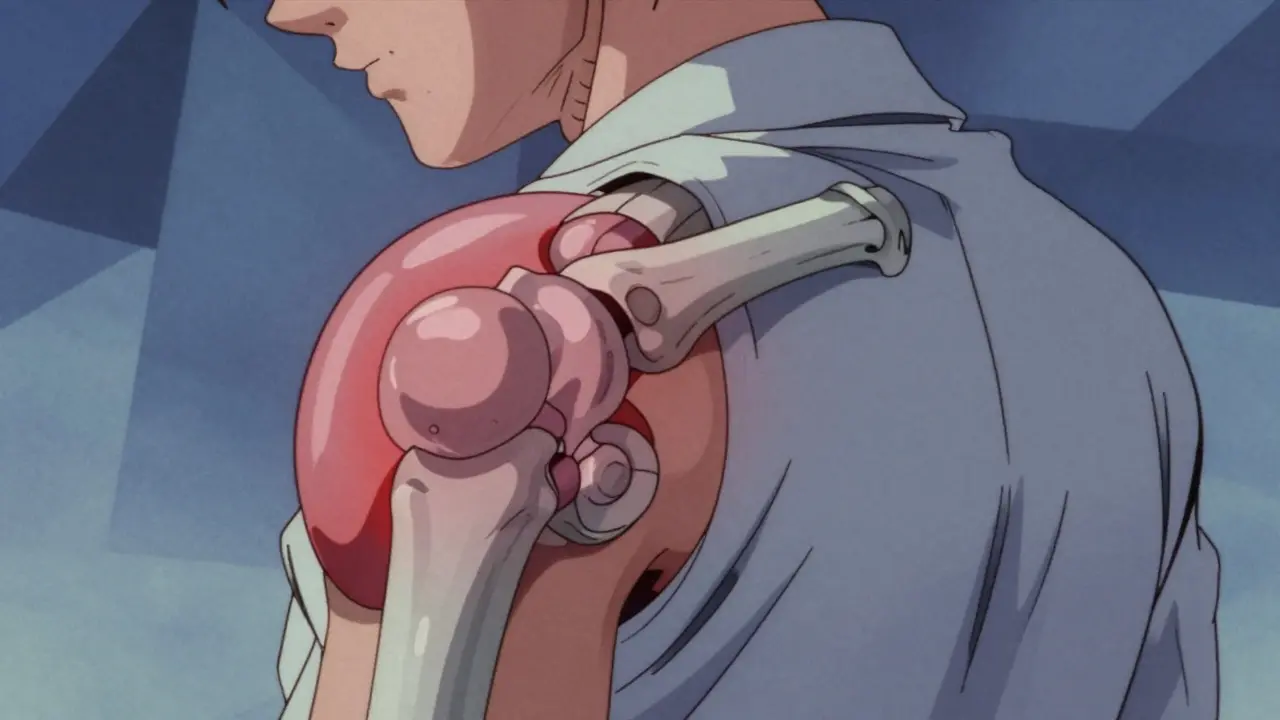
To treat frozen shoulder effectively, you first need to understand what it is. Despite the name, there are rarely actual "adhesions" or glue-like bands holding the joint together. Instead, the pathology involves severe inflammation and fibrosis of the shoulder joint capsule. Specifically, the antero-superior part of the capsule, the axillary recess, and the coracohumeral ligament become inflamed and shrink.
Think of the shoulder capsule like a balloon. In a healthy shoulder, this balloon has plenty of room for the ball of the upper arm bone to move freely. In adhesive capsulitis, that balloon shrinks by about 45%. Studies show the volume drops from a normal 30-35 mL to just 10-15 mL. This lack of space creates the classic "capsular pattern" of restriction:
- External Rotation: Most affected (60-70% limitation). You struggle to turn your palm away from your body.
- Abduction: Second most affected (50-60% limitation). Lifting your arm out to the side is difficult.
- Internal Rotation: Least affected but still limited (40-50% limitation). Reaching behind your back is tough.
This condition affects 2-5% of the general population. However, if you have diabetes, your risk jumps to 10-20%. The stiffening happens because the body’s inflammatory response goes into overdrive, creating scar tissue that restricts movement. Understanding this biology helps explain why aggressive stretching too early can backfire-it irritates the inflamed tissue rather than loosening it.
The Three Stages of Frozen Shoulder
Frozen shoulder is not static; it evolves. Recognizing which stage you are in dictates your treatment strategy. Treating the freezing phase like the thawing phase is a common mistake that leads to increased pain.
- The Freezing Stage (Painful Phase): Lasts 6 weeks to 9 months. Pain is the dominant symptom, especially at night. Range of motion begins to decrease slowly. During this time, the goal is pain management and maintaining whatever motion you have left without aggravating inflammation.
- The Frozen Stage (Stiff Phase): Lasts 4 to 6 months. The pain may subside, but stiffness becomes severe. This is when the "frozen" sensation is most pronounced. Active and passive range of motion are equally restricted. This is the prime window for more aggressive mobilization.
- The Thawing Stage (Recovery Phase): Lasts 6 months to 2 years. Range of motion gradually returns. Pain is minimal. The focus shifts to strengthening the muscles around the shoulder to support the newly regained mobility.
A systematic review published in the American Family Physician (2019) highlights that intervention timing matters. Starting gentle mobilization during the freezing phase can prevent excessive contracture, while waiting until the frozen stage allows for more intensive stretching.
Mobilization Strategies: Exercises That Work
Mobilization does not mean forcing your arm through pain. It means guided, progressive movement. Here are the most effective, evidence-based strategies used by physical therapists.
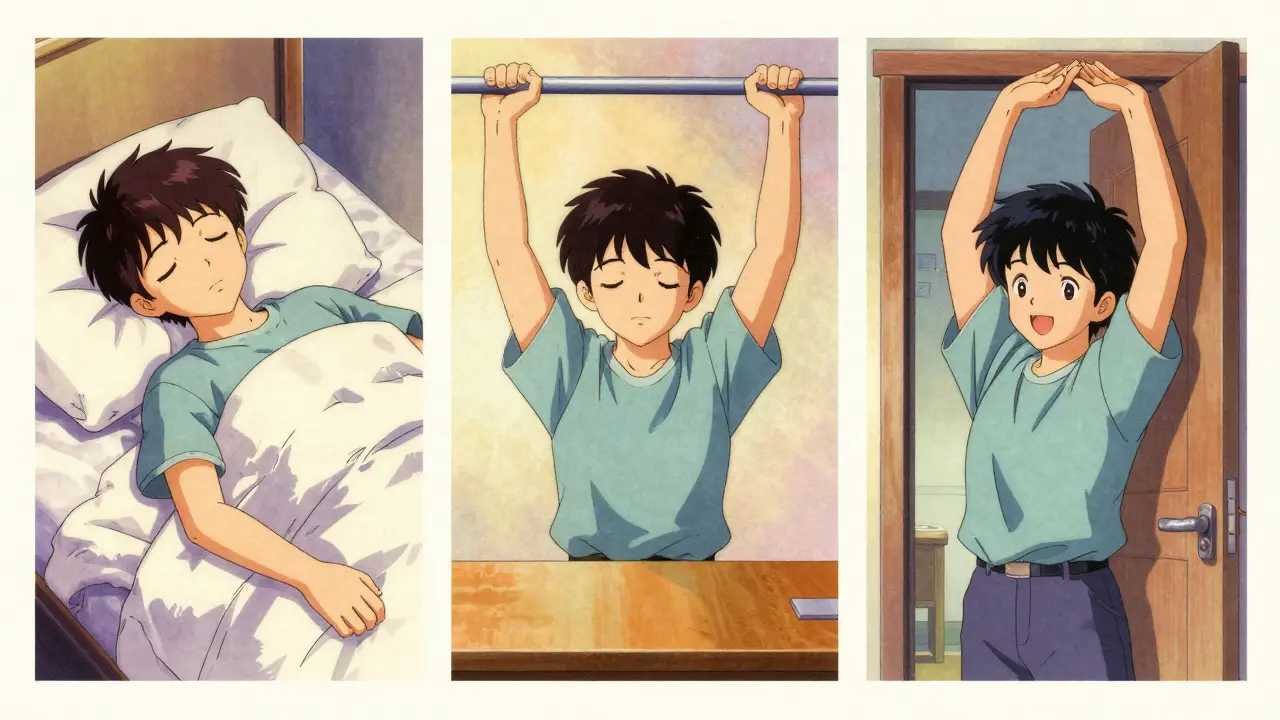
Pendulum Exercises (Codman’s Exercises)
These are ideal for the freezing phase. Lean forward, supporting your weight with your unaffected arm on a table. Let the affected arm hang loose like a dead weight. Gently swing your body to create small circles with the hanging arm. Gravity does the work, not your muscles. This lubricates the joint without stressing the tightened capsule. Aim for 5 minutes, twice daily.
Towel Stretch
This targets internal rotation. Hold a towel behind your back with both hands. Use your unaffected hand to pull the towel upward, gently lifting the affected hand. Stop at the point of tension, not sharp pain. Hold for 15-30 seconds. Repeat 10 times. This is crucial for restoring the ability to reach behind your back.
Doorway Stretch
Stand in a doorway. Place your forearms on the doorframe at shoulder height. Gently lean forward until you feel a stretch across the front of your shoulders and chest. This addresses the anterior capsule tightness. Hold for 30 seconds. Repeat 3-5 times.
Cross-Body Adduction
Use your unaffected arm to lift the affected arm across your chest. Pull it gently toward your body. This stretches the posterior capsule. Be cautious: if you are in the acute freezing phase, this can increase pain. Consult a therapist before attempting this if pain is high.
| Exercise | Best For Stage | Primary Target | Risk Level |
|---|---|---|---|
| Pendulum | Freezing | Joint Lubrication | Low |
| Towel Stretch | Frozen / Thawing | Internal Rotation | Medium |
| Doorway Stretch | All Stages | Anterior Capsule | Low |
| Cross-Body | Frozen / Thawing | Posterior Capsule | High (if acute) |
Differentiating Frozen Shoulder from Other Conditions
Many people assume any shoulder pain is a rotator cuff tear. Misdiagnosis rates in primary care are estimated at 30-40%. How do you tell the difference?
In a rotator cuff tear, your active range of motion (moving your arm yourself) is limited due to weakness or pain, but your passive range of motion (someone else moving your arm) is usually preserved. In frozen shoulder, both active and passive motion are globally restricted. If you cannot lift your arm even when someone else helps you, it points strongly to adhesive capsulitis.
Additionally, frozen shoulder typically presents with an insidious onset-no major trauma, just gradual worsening. Red flags like fever, unexplained weight loss, or night sweats suggest systemic issues like infection or cancer, requiring immediate medical attention beyond simple mobilization.
Managing Pain and Nighttime Discomfort
Night pain is reported by 78% of patients. It disrupts sleep, which hinders healing. Simple positioning changes can help:
- Sleep on your back: Place a pillow under the affected arm to keep it slightly elevated and supported.
- Sleep on the unaffected side: Hug a pillow against your chest to support the affected arm, preventing it from falling backward and stretching the tight capsule.
- Avoid stomach sleeping: This forces the shoulder into extreme external rotation, aggravating the condition.
Heat application before exercises increases blood flow and tissue elasticity. Ice after exercises can reduce post-movement inflammation. Consistency is key-doing these small things daily adds up to significant progress.
When to Seek Professional Help
While home exercises are vital, supervised physical therapy offers a 28% faster recovery rate compared to home programs alone, according to AAOS guidelines. A physical therapist can provide manual therapy techniques that you cannot replicate at home, such as joint glides and capsular stretching.
If conservative management fails after 6 months, interventions like corticosteroid injections may offer short-term pain relief (4-8 weeks), allowing you to participate more effectively in therapy. In rare cases (13% of persistent cases), surgical options like manipulation under anesthesia or arthroscopic capsular release may be considered. However, surgery is always a last resort.
Remember, frozen shoulder is a marathon, not a sprint. Patience, consistency, and smart mobilization are your best tools. Start gently, listen to your body, and trust the process.
How long does frozen shoulder last without treatment?
Without targeted mobilization, frozen shoulder can last 1 to 3 years, and in some cases up to 11 years. The condition is self-limiting, meaning it resolves on its own, but the prolonged duration causes significant functional impairment and quality of life issues.
Can frozen shoulder go away on its own?
Yes, frozen shoulder is a self-limiting condition. However, "going away" does not mean returning to full function quickly. Without intervention, the recovery timeline is significantly longer, and some residual stiffness may remain. Early mobilization speeds up the process and improves outcomes.
What is the best exercise for frozen shoulder?
The best exercise depends on the stage. In the freezing phase, pendulum exercises are safest. In the frozen and thawing phases, towel stretches and doorway stretches are highly effective for regaining range of motion. Consistency with a combination of these exercises yields the best results.
Is frozen shoulder caused by injury?
Usually, no. Primary adhesive capsulitis occurs without a clear cause, though it is linked to diabetes, thyroid disorders, and cardiovascular disease. Secondary frozen shoulder can follow immobilization due to injury (like a fracture or stroke), but the initial event is the lack of movement, not the injury itself causing the capsular tightening directly.
Should I push through the pain during exercises?
No. You should stretch to the point of tension or mild discomfort, but never sharp pain. Pushing through sharp pain increases inflammation, which can worsen the condition and prolong recovery. Gentle, consistent stretching is more effective than aggressive, painful force.

11 Comments
you really think people need a whole essay to tell them not to push through pain. it is obvious that forcing your arm hurts but here we are reading paragraphs about it anyway
I found the section on differentiating between rotator cuff tears and frozen shoulder particularly useful. Many people confuse the two because both involve limited movement, but the distinction between active and passive range of motion is crucial for proper diagnosis. It would be beneficial to consult a specialist if you are unsure which condition you are dealing with.
This is very helpful information. I had this issue last year and it was really tough. The towel stretch helped me a lot in the end. Just remember to take it slow. Do not rush the process or you will hurt yourself more. Keep going every day even if it feels hard.
ugh another medical post telling us what to do with our bodies like we do not know better :/ i have been doing these stretches for months and nothing changes so why should anyone else bother. maybe if you just ate more kale it would go away lol
It is quite fascinating, indeed, how the body can betray us in such specific ways, yet the advice provided here seems rather generic, does it not? One must consider that every individual’s physiology is unique, and therefore, a one-size-fits-all approach to rehabilitation is inherently flawed, despite the best intentions of the author, who clearly believes they have discovered the ultimate solution to a complex biological puzzle that has baffled physicians for centuries.
The methodology described herein is acceptable, albeit simplistic. It is imperative that individuals adhere strictly to the prescribed protocols without deviation. Failure to comply with the recommended stretching regimens will result in prolonged suffering, which is entirely self-inflicted due to a lack of discipline and respect for medical guidance.
i disagree with the part about heat application. ice works better for inflammation usually. also the timeline seems too optimistic for most people. mine took forever to heal and no amount of stretching fixed it quickly
I appreciate the detailed breakdown of the three stages. Understanding whether you are in the freezing, frozen, or thawing phase is critical because the treatment approach varies significantly between them. For those in the early painful stage, focusing on pain management rather than aggressive stretching is key to preventing further inflammation. Have you found any specific techniques that help with the night pain mentioned in the article?
hey guys dont give up on this stuff! i knwo it sucks but trust the process man. my physio said consistency is king. try the pendulum exercises first thing in the morning. it helps get the blood flowing. keep pushing forward and stay positive u got this!
Wow, this is incredibly comprehensive! I am currently in the frozen stage and it has been so frustrating to see my range of motion decrease despite the pain subsiding. The tip about hugging a pillow while sleeping on the unaffected side is a game-changer. I have been struggling to sleep comfortably, so this simple adjustment might finally help me get some rest. Thank you for sharing such practical advice!
Oh, how delightful that we must now treat our shoulders like delicate porcelain dolls rather than robust joints designed for labor. In my village, we did not have time for 'pendulum exercises' when we were working the fields from dawn till dusk. Perhaps if people spent less time sitting at computers and more time engaging in actual physical activity, this 'epidemic' of frozen shoulders would vanish. But no, let us all gently swing our arms like clockwork instead of living life.